At flytospine.com, we are always looking for the most advanced and effective options for your spine care. Today we are going to explore a surgical approach for isthmic spondylolisthesis that is gaining ground for its benefits for both the patient and the surgeon: pure anterior fusion or standalone ALIF.
A Look at Isthmic Spondylolisthesis and Its Evolution in Treatment
Isthmic spondylolisthesis is a condition in which a vertebra in the lumbar spine slips forward over the lower vertebra. This occurs due to a fracture or defect in a small part of the bone called the isthmus or pars interarticularis, often the result of repetitive stress, common in athletes. Although it can be asymptomatic, when it causes persistent low back pain, leg pain, or neurological deficits that do not improve with conservative treatments, surgery becomes an option.
Historically, the treatment of spondylolisthesis has evolved significantly. From the first descriptions in the 18th century, through the identification of the entity in the 20th century, surgical techniques have advanced remarkably. Initially, procedures such as isolated neural decompression were popular, but often resulted in further progression of the slip due to lack of fusion. Posterolateral fusion (PLF) was described in the early 20th century and required long immobilizations since implants were not used to stabilize and hold the vertebrae.
The real breakthrough came with the development of spinal instrumentation, such as pedicle screws, devised in the 1970s by the American surgeon Arthur Steffee and improved for deformity techniques in the 1980s by the Frenchmen Yves Cotrel and Jean Duboisset. In the 1990s, interbody cages as we know them today appeared, allowing for more stable and effective fusion techniques, such as TLIF (Transforaminal Lumbar Interbody Fusion), described by the German Jurgen Harms. In the 21st century, spine surgery has embraced innovation, with minimally invasive approaches, advanced implants, and robotics-assisted systems that improve precision and recovery while reducing morbidity. It is in this context of constant improvement that standalone ALIF has resurfaced strongly.
What is Standalone ALIF and Why is it Different?
Anterior Lumbar Interbody Fusion (ALIF) is a fusion technique performed by accessing the spine through a small incision in the abdomen, at the front of the body. Unlike traditional posterior approaches, which require working through the back muscles, ALIF allows the surgeon to reach the spine without disturbing the posterior musculature and ligaments.
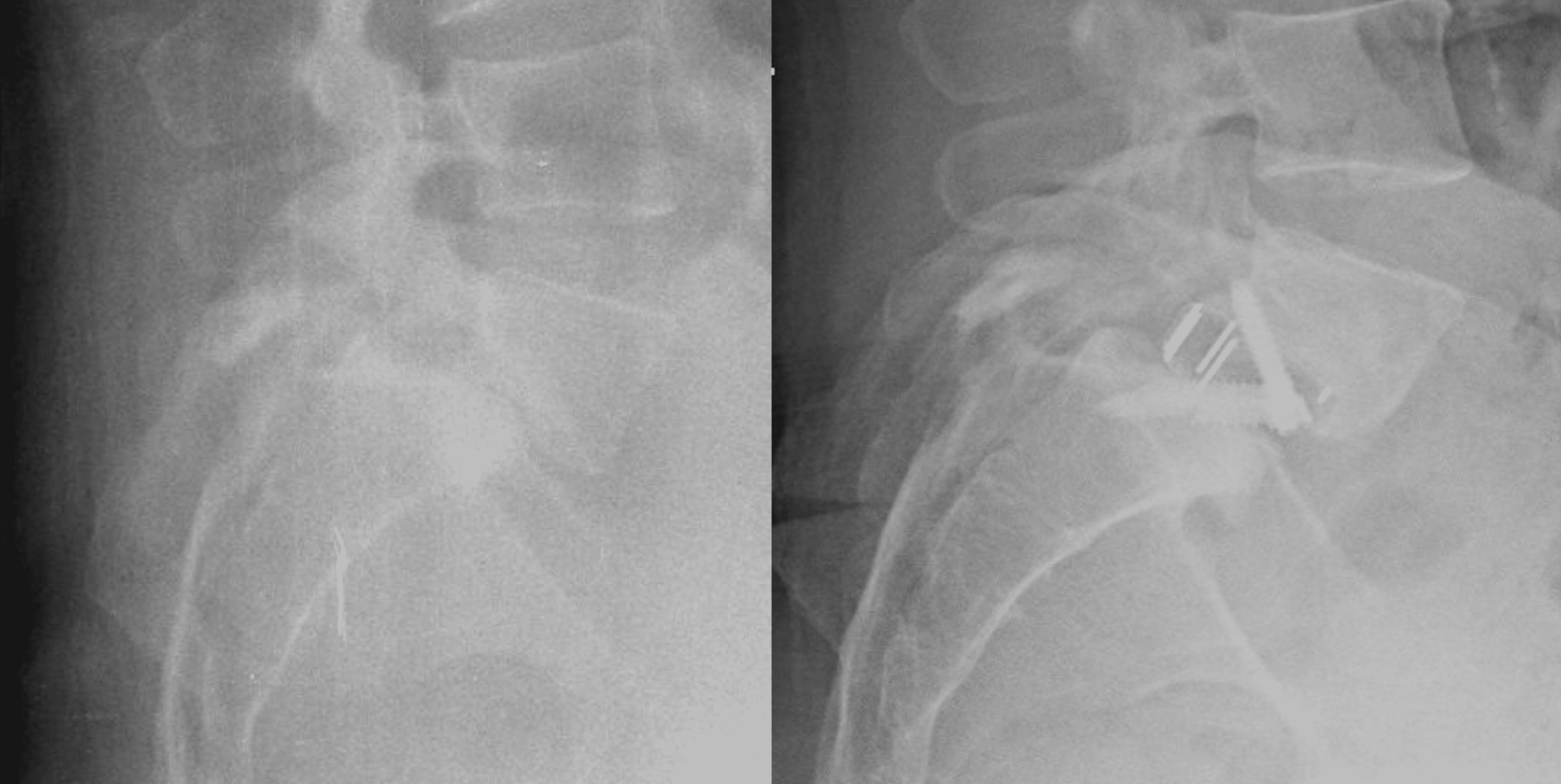
The term “standalone” means that fusion is achieved using only one implant (a cage or spacer) inserted into the disc space, often with screws or a plate integrated into the implant itself, without the need to add additional posterior instrumentation, such as pedicle screws in the back. This contrasts with ALIF-PSF (ALIF with supplemental posterior fixation), which combines the anterior approach with screws placed from the back to ensure stability.



Advantages of Standalone ALIF: Benefits for Patient and Surgeon
The case for standalone ALIF in the 21st century is based on solid medical and biomechanical justifications, which translate into tangible benefits:
For the Patient: Better Quality of Life and Recovery
- Less Invasive and Less Postoperative Pain: By avoiding dissection of the large back muscles, standalone ALIF reduces posterior muscle and ligament damage. This translates into less postoperative pain, potentially faster recovery, and absence of long-term muscle atrophy.
- Accelerated Recovery: Patients are usually walking within a few hours or the day after surgery and can return to normal activities in as little as six weeks, depending on the type of work. The hospital stay is 1 to 3 days, but discharge within 24 hours is very common.
- Indirect Neural Decompression: The ALIF technique allows for the insertion of a larger interbody cage into the disc space. This not only restores disc height but also indirectly increases the space for the nerve roots (foramen), relieving compression without the need for direct posterior decompression, which carries its own risks.
- Restoring the Natural Curvature of the Spine: The ability to insert larger implants with controlled angulations from the front helps restore the natural curvature (lordosis) of the lumbar spine, which is very beneficial for stability and posture and, therefore, for the final result.
- Slip Correction: Although the anterior approach did not grant a direct capacity to perform slip reduction maneuvers, the truth is that mere distraction and increase in disc space already produces a reduction effect of one grade in most cases. In addition, we have latest-generation implants that also allow adding another degree of reduction (about 8 mm) through a sliding drawer mechanism.
For the Surgeon: Technical Advantages and Efficiency
- Direct and Wide Access to the Disc: The anterior approach provides a clear view and unobstructed access to the disc space, allowing for complete removal of the damaged disc and precise placement of large implants.
- Greater Construct Stability: The insertion of a large cage spanning a wide surface area of the vertebral endplates, together with compression of the bone graft, contributes to the inherent stability of the fusion construct.
- Reduction of Surgical Times and Costs: By eliminating the need for a second posterior approach and associated instrumentation, standalone ALIF drastically reduces surgery time and overall procedure costs. This is a benefit for both the health system and the patient.
Who is an Ideal Candidate for Standalone ALIF?
The key to the success of standalone ALIF lies in rigorous patient selection. This approach is especially promising for:
- Symptomatic Grade I and II Isthmic Spondylolisthesis: Patients with low-grade slips who experience persistent pain and do not respond to conservative treatments.
- Good Bone Quality: It is fundamental that patients have normal bone density to ensure integration and stability of the implant.
- Adequate Sacral Slope: A sacral slope below 40° is a favorable factor. Highly lordotic columns with a very tilted sacral plate can transmit a lot of shear force to the implant screws, increasing the risk of breakage.
- Body Mass Index (BMI) <35: A high BMI can increase surgical complexity and the risk of complications.
Conclusion: A Promising Future for Your Spine
Anterior Lumbar Interbody Fusion (ALIF) in its standalone modality represents a significant advance in the treatment of low-grade isthmic spondylolisthesis. By combining a less invasive surgical technique with clinical and radiographic results comparable to more extensive approaches, it offers a promising pathway to improve quality of life, speed recovery, and optimize results for suitable patients.
If you suffer from persistent back pain due to isthmic spondylolisthesis, we encourage you to consult with a spine specialist. An accurate diagnosis and a detailed discussion of all treatment options, including standalone ALIF, are the first step toward a healthier spine and a pain-free life.

