The Degenerative Cascade and the Concept of Instability
The lumbar spine is a biomechanically complex structure where disc degeneration represents the onset of a series of pathological changes that Kirkaldy-Willis termed the “degenerative cascade.” This process, affecting millions of individuals worldwide, typically evolves through three phases: initial dysfunction, instability, and ultimately restabilization. It is precisely the instability phase that generates the greatest scientific debate and therapeutic controversy.
The Concept of Segmental Instability
Lumbar segmental instability represents one of the most debated concepts in spine surgery. Biomechanically defined as abnormal motion of the vertebral segment under physiological loads, its clinical diagnosis remains elusive. White and Panjabi proposed specific radiological criteria, yet the correlation between imaging findings and clinical symptoms is far from perfect.
Patients with segmental instability typically present with mechanical low back pain that worsens with activity and improves with rest. However, distinguishing this pain from that caused by other degenerative pathologies constitutes a considerable diagnostic challenge.
The Birth of Dynamic Stabilization
Conceptual Origins
The idea of preserving motion while providing stabilization emerged as a response to the limitations observed with traditional spinal fusion. Surgeons noted that while arthrodesis achieved pain relief in many patients, it also completely eliminated motion at the treated segment, transferring additional loads to adjacent levels.
The concept of “dynamic stabilization” or “flexible fixation” arose from the observation that perhaps it was not necessary to eliminate all motion to achieve symptomatic relief. The hypothesis was that controlling excessive motion while maintaining some residual mobility would suffice.
Gilles Dubois and the Genesis of Dynesys
In the 1990s, Swiss engineer Gilles Dubois, working in collaboration with European spine surgeons, developed the Dynesys (Dynamic Neutralization System). His revolutionary design consisted of titanium pedicle screws connected by a polycarbonate-urethane spacer and a polyethylene terephthalate cord.
The biomechanical principle was elegant: the spacer resisted compression while the cord limited distraction and excessive flexion. Theoretically, this allowed a controlled range of motion, avoiding the extreme positions that generated pain without the need to fuse the segment.
The Rise of Dynesys
Initial Promise and Enthusiasm
The Dynesys system received CE marking in Europe in 1998 and generated considerable enthusiasm within the spine surgery community. Early studies published by Stoll, Dubois, and Schwarzenbach showed promising results, with significant improvements in pain and functional outcome scores.
The surgical technique was relatively straightforward for surgeons familiar with pedicle screw systems. A traditional posterior approach was performed, pedicle screws were placed, and they were connected with the spacer and cord system.
Proposed Indications
Proponents of the system suggested multiple indications:
- Disc degeneration with documented instability
- Spinal stenosis with an instability component
- Recurrent disc herniation
- Post-laminectomy syndrome
- Prevention of adjacent segment degeneration following fusion
Global Adoption
The system was adopted by numerous centers throughout Europe, Asia, and subsequently the United States, where it received FDA approval in 2009, although specifically as a posterior fusion system, not as a motion-preservation device.
Problems Emerge
Mechanical Failures
As clinical experience accumulated, significant complications began to be reported. The polycarbonate-urethane spacers showed degradation over time, and cases of polyethylene cord rupture were documented.
Stucki and colleagues published a case series with mechanical failures requiring surgical revision. The rate of mechanical complications varied between 5% and 17% across different series—a concerning figure for a device designed as a less invasive alternative to fusion.

Does It Actually Preserve Motion?
More detailed biomechanical studies revealed that the Dynesys system reduced segmental motion more than initially theorized. Kinematic analyses showed that, in many cases, residual motion was minimal, questioning the fundamental premise of the device.
Furthermore, several studies with extended follow-up documented that many segments treated with Dynesys eventually fused spontaneously. If the final outcome was fusion, what advantage did it offer over planned arthrodesis?
Adjacent Segment Degeneration
One of the primary justifications for dynamic stabilization was the prevention of adjacent segment degeneration (ASD). However, comparative studies failed to demonstrate a clear advantage over traditional fusion in this regard. Kumar’s systematic review showed similar ASD rates between both techniques.
The OSTEO Trial: The Final Blow
The OSTEO study, a prospective multicenter clinical trial comparing Dynesys with posterolateral fusion, was published with disappointing results. At two-year follow-up, no significant differences in clinical outcomes were demonstrated between groups, while the Dynesys group showed a higher reoperation rate.
This study, along with the accumulation of negative evidence, marked the definitive decline of the system in routine clinical practice.

The Wiltse Approach: A Technique That Endures
Leon Wiltse and Muscle Preservation
While the debate over dynamic stabilization reached its peak, a surgical technique developed decades earlier demonstrated its enduring value. Leon Wiltse, a California orthopedic surgeon, described in 1968 a paraspinal approach to the lumbar spine that minimized damage to the extensor musculature.
The traditional midline approach, described by Hibbs in 1911, required extensive denervation and detachment of the paravertebral muscles to access posterior structures. Wiltse observed that this generated persistent weakness, muscle atrophy, and chronic postoperative pain in many patients.

The Paraspinal Approach Concept
The Wiltse approach utilizes a natural intermuscular plane between the multifidus and longissimus muscles. By following this avascular plane, the surgeon can access the vertebral pedicles with minimal muscular disruption.
The theoretical advantages were evident:
- Reduced intraoperative blood loss
- Preservation of muscular innervation
- Less immediate postoperative pain
- Better functional recovery
- Reduction in failed back surgery syndrome
Scientific Validation
Unlike dynamic stabilization, the Wiltse approach has accumulated decades of favorable evidence. Comparative studies have consistently demonstrated less atrophy of the paravertebral muscles when this approach is utilized.
Kim’s group published magnetic resonance imaging studies demonstrating preservation of multifidus cross-sectional area with the paraspinal approach compared to the midline approach. Stevens and colleagues documented better long-term functional outcomes.
Modern Application
In current practice, the Wiltse approach is used for:
- Pedicle screw placement in fusion procedures
- Percutaneous fixation surgery
- Lateral decompression procedures
- Vertebral fracture repair
The technique has proven particularly valuable in minimally invasive surgery, where muscle preservation principles are fundamental.
Transition: The Successor to Dynesys
Design and Concept
Given the evident limitations of Dynesys, the spinal device industry developed next-generation systems. Transition (Globus Medical) represents a conceptual evolution that attempts to maintain the theoretical benefits of dynamic stabilization while addressing its mechanical weaknesses.
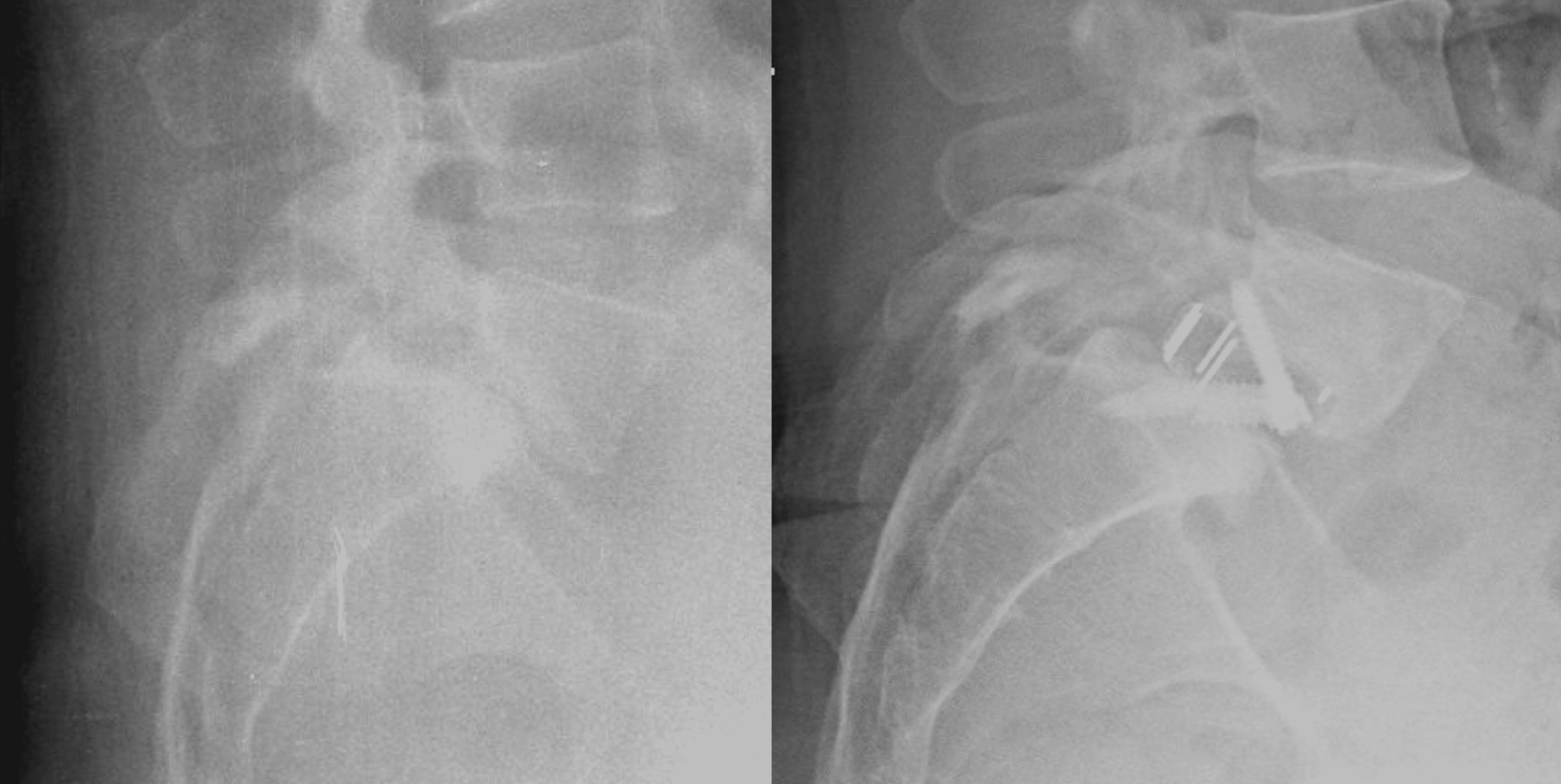
The system uses pedicle screws with articulating heads that allow a degree of controlled motion. Unlike Dynesys, Transition employs more resistant metallic materials and a design that allows adjustment of the degree of motion restriction.


The TRANSITION™ Stabilization System: lateral and anteroposterior views
Available Evidence
The literature on Transition is considerably more limited than that existing for Dynesys. Published studies are primarily case series with short follow-up and without comparison to established techniques.
Proponents argue that the improved design avoids the mechanical problems of its predecessor, but the scientific community maintains a healthy skepticism given the historical precedent.
Current Position in Clinical Practice
Adoption of next-generation dynamic stabilization systems remains limited. Most spine surgeons prefer established techniques with robust evidence: fusion when indicated, or conservative management when not.
The niche for these devices, if it exists, appears to be highly specific: young patients with symptomatic disc degeneration and clear evidence of instability who wish to avoid fusion and accept uncertainty regarding long-term outcomes.
The Regulatory Paradox
Approval vs. Evidence
The history of Dynesys illustrates a persistent problem in medical device regulation. The system received CE marking in Europe based on short-term safety studies, without the need to demonstrate comparative efficacy against established treatments.
In the United States, the FDA approved Dynesys specifically as a fusion system, not as a motion-preservation device, implicitly recognizing the lack of evidence for its promoted indication.
Implications for Innovation
This case raises fundamental questions about the balance between innovation and patient protection. Should a new device demonstrate superiority over established treatments before being commercialized? Or is it sufficient to demonstrate basic safety?
Advocates of stricter regulation argue that thousands of patients were treated with a device that never demonstrated advantages over established alternatives. Innovation advocates note that delaying the availability of new technologies also has costs.
Lessons for the Future
Biomechanics vs. Biology
A fundamental lesson from the dynamic stabilization experience is the discrepancy between theoretical biomechanical concepts and complex biological reality. The mechanical model of the spine as a structure of bars and hinges is useful but incomplete.
Living tissues respond to mechanical stress in complex and unpredictable ways. The ossification of “dynamically stabilized” segments demonstrates that biology has its own imperatives that transcend engineering designs.
The Importance of Extended Follow-Up
The promising short-term results with Dynesys did not translate into lasting benefits. This underscores the need for studies with extended follow-up before widely adopting new technologies.
In spine surgery, where patients live for decades with the results of their interventions, two-year follow-up is insufficient to establish efficacy.
Comparative Evidence
The lack of rigorous comparative studies allowed Dynesys to be widely adopted before its actual efficacy could be evaluated. The OSTEO trial arrived years after thousands of patients had been treated.
Healthcare systems must require comparative evidence before incorporating new technologies, especially when established alternatives exist.
Current Status and Perspectives
Dynamic Stabilization Today
The concept of dynamic stabilization has not completely died. Some centers continue to use these systems in selected cases, and research continues exploring improved designs.
However, the enthusiasm of the early 21st century has transformed into well-founded caution. The spine surgery community has learned to be skeptical of promises from technologies that “preserve motion” without robust evidence.
The Future of Motion Preservation
Other motion-preservation technologies, such as artificial disc replacement, have shown more promising results in the cervical segment. In the lumbar spine, results are more heterogeneous.
Current research focuses on improved patient selection criteria, combining clinical, imaging, and biomarker data to identify those who might benefit from these technologies.
The Wiltse Approach: An Enduring Legacy
In contrast to the Dynesys story, the Wiltse technique represents the type of innovation that endures: based on solid anatomical and physiological principles, gradually validated by accumulated evidence, and adopted because it consistently improves patient outcomes.
The muscle preservation that Wiltse advocated over 50 years ago is now a fundamental principle of modern spine surgery, incorporated into minimally invasive techniques that continue to evolve.
Conclusions
The history of lumbar dynamic stabilization, from the initial enthusiasm for Dynesys to its decline and the search for alternatives, offers valuable lessons for contemporary medical practice. It illustrates both the dangers of premature enthusiasm for new technologies and the importance of rigorous evidence.
The Wiltse approach, in contrast, demonstrates that the most enduring innovation often arises from careful observation and respect for anatomy and physiology, rather than from revolutionary devices.
For patients with lumbar instability, the current message is one of informed caution: effective treatment options exist, both conservative and surgical, but promises of technologies that “do everything” must be critically evaluated in light of available evidence.
The spine remains a complex biomechanical and biological system that regularly humbles attempts at simplistic technological solutions. The modern spine surgeon must combine knowledge of proven traditional techniques with the ability to critically evaluate emerging innovations.
Ready to Discuss Your Spine Condition?
If you’re experiencing chronic back pain or have been diagnosed with lumbar instability, Dr. Diego Ferrández offers remote consultations for international patients.
Get expert guidance from one of Spain’s leading spine surgeons — from the comfort of your home.
Book Your Teleconsultation Now →
Available in English and Spanish. Secure video consultation with detailed written report included.